On the Frontline (Muhammad Eyad Ba’Ath)

Syria is so extensively covered in the media nowadays, for mostly the wrong reasons, that I no longer need to explain where my home country is in response to the very usual and old question of “where are you from?” Rather, I need to ignore the suspicious and fearful looks generated by my answer. During the Scotland referendum in 2014, I clearly remember Syria having the dubious distinction of being more talked about on Radio 4 than the rather trivial and insignificant issue of the UK splitting in half and losing the very essence of its name. Regardless of this and beyond the usual coverage (we all know the numbers … 800 or so went, half came back … etc), this is a country of originally 23 million people that is still going through 6 years and counting of full-scale war. This is as long as the entire Second World War. It has been suggested that 3% of the population have been killed, 10% injured and almost half displaced internally, parked in camps in neighboring countries or taken the smugglers’ option of a no-visa excursion to Greece and the European Community. In absolute numbers the impact of the war on Syria has been bigger than the impact of either world war on the UK. Syria is also far from being isolated. The biggest influx of Syrians into Europe happened during the last few years (Germany alone received about 800,000). The other aspect of the conflict that does not get much media coverage is the extensive and excellent work done by a network of UK-based charities, some well known and others less so.

I arrived at Alder Hey Hospital in Liverpool in 2003 as an overseas, possibly naïve, surgical trainee. At that time I came from a very stable but rather exotic and obscure middle-eastern country of Syria. There was not much in the way of democracy, being led by members of the al-Assad clan; Hafiz al-Assad before 2000 and currently Bashir his son since. But I could never have imagined where I would be today and in what circumstances. Life is truly very strange.
The desperate need for doctors was obvious to me following two previous visits to Syria during the conflict. The doctor-to-population ratio has dropped considerably and is currently estimated at <2 per 10,000 population (the UK has about 28 per 10,000). I had finished my training in 2014 and then did a short period as consultant at Alder Hey. After this, I decided to move back to my homeland. The reasons were rather complex but the more the time goes by the more it feels it just happened and the explanations are less clear in my mind. The risks were then and still are considerable, of course. There is the repeated targeting of medical facilites with the aim of shutting them down, and being the unwanted focus of various governmental and other “agencies”, to working with what limited resources exist. All of these are things that you might experience daily in the NHS but Syria brings to it a rather different scale. I’d still consider the difference one of magnitude rather than type. However, all the above is still a mere inconvenience when compared to the stress generated by operating on a sick kid or having a significant complication. I know most of my readers would identify with this statement, even in my current circumstances this is the thing that mostly keeps me up at night.
[caption id="attachment_9497" align="aligncenter" width="648"] Panoramic view of Bab Al Hawa Hospital[/caption]
Panoramic view of Bab Al Hawa Hospital[/caption]
I moved to Bab-Al Hawa Hospital (معبر باب الهوى, “Gate of the Winds”) almost two and a half years ago and established my very own paediatric surgical unit. The hospital is the largest medical facility in areas outside regime control and services a population of probably 5 million and is completely free at the point of delivery. It is located “on” the international Turkish-Syrian border with the hope that this would make it less likely to be targeted by the devastataion of barrel bomb attack since regime helicopters would try to stay out of Turkish air space.The department currently has a neonatal surgical unit of 6 incubators and a ward of 11 beds. Despite a recent expansion, our bed occupancy rate still stands at more than 85% and we often spill into other sections of the hospital. I cover the department for 20 days a month and my week is fully packed: 5 theatre days, 1 clinic day and a day in the endoscopy suite where I do PEGs, oesophageal dilatation and diagnostic OGDs. This is in addition to covering emergencies -including traumas round the clock. I have a “month-end” instead of a “week-end”. We are incredibly busy in terms of both volume and index cases.

I do easily in excess of 100 cases a month and more than 70% of our patients are under 3 years of age. During the first month following official openning we had 6 oesophageal atresias (Alder Hey perhaps gets around 10 a year). I had a month where I operated on 3 cloacal anomalies and another where I operated on 4 exstrophies. I probably do a two-stage hypospadias every fortnight and a PSARP or some form of pull-through at least once a week. We also have a laparoscopy stack and I have done laparoscopic fundoplications, splenectomies and diaphragmatic hernia repairs. My logbook also contains oesophageal replacements, closing acquired recto-vaginal and urethral fistulas and feminising genitoplasties in addition to other rarities. The busiest part of the job however is the “whats app” clinic that is open 24/7 where you get approached by random patients for random complaints. This is where you are still a paediatric surgeon but filling in the role of NHS Direct or a secretary. While very useful and convenient at times the worst part of it is that you are never truly “off work”.
As you can tell the work can be exhausting but generally very rewarding. For someone who likes being in theatre it is a dream job. I don’t have the luxury -or annoyance- of subspecialisation. I have even been forced to develop new skills like treating cleft lip and palate and handling ventilators. My practice is probably the ultimate application of the often repeated statement of paediatric surgery being “the last bastion of general surgery”. The job has obvious risks and drawbacks but does have some perks: you become a local hero and a bit of a celebrity. Not a week goes by without an inviation to a feast or getting a present – usually seasonal land produce. As people know you are there to share and hopefully alleviate their hardship you get connected to them on a level you would never achieve in the NHS since it might jeopardize your professionalism. For example, sometimes assuming a paternalistic approach is important, telling some parents off to achieve a desired outcome and improvement in their child and usually they would be grateful for it and without complaint. At times I wish I had colleagues that I could simply ask a second opinion from and with that regards maintaining a link with the UK has been great help but it will never be like having someone with me on the ground. It can be tough at times but I do not regret it at all. There is a lot of political uncertainity so we tend to focus on the rather near future but I guess in today’s world this is not out of the norm.
Within our setup there are conditions that have less than optimal outcome. These generally include neonatal cases that need parenteral nutrition such as small bowel atresias with reduced bowel length and cases of gastroschisis. Long-term ventilator support for diaphragmatic hernias and oesophageal atresia is difficult. Most other patients we treat do have good outcome and mortality is generally <2% of total admissions (neonates are over-represented). We have had consistent improvement over time and since enforcing hand hygiene our infection rates (the biggest killer) have significantly dropped. If I’m to start all over again I’d completely isolate the neonatal unit and enforce a bare-below the elbow and hand hygiene policies from Day 1.
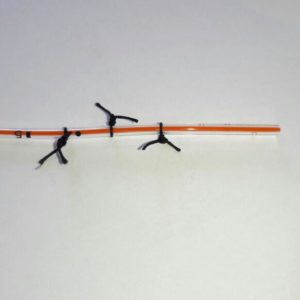
On the positive side as well is my series of little “innovations” , if I’m allowed to describe them as such. which I was forced to come up with. A good example of this is the Trans-Nasal Trans-Pyloric Suture Guided Peristalsis Powered Hand-Made Feeding Jejunostomy or TNTPSGPPHMFJ for short. While I will lay claim to the intellectual thought behind this “invention” I guess it is not original. It consists of putting silk ligatures around the end of a 5 Fr feeding tube (see picture). The silk sutures provide a latching point for intestinal peristalsis and drive the tip of the tube distally ideally to the jejunum where it can be used for feeding. It is, in my experience, a good way of managing a vomiting child, especially when you are unsure about the diagnosis. Cases when I failed to intubate the small bowel usually turn out to be pyloric stenosis so it does have some diagnostic merit as well.

In my other attempts at “maintaining standards” I have also tried to replace some costly equipment with cheaper alternatives. Examples include the handmade pre-made silo for gastroschisis which is made of a silastic drain tube and a urine collection bag with some 3-0 Prolene™ sutures, the hand-sewn BairHugger™ blanket, the CPS (that’s Cheap Pena Stimulator) which is simply a nerve stimulator device adapted for use in anorectal malformation. I have also came up with a sequel to the Noblett rectal biopsy “Gun” which is the Ba’Ath rectal biopsy “Bullet” … as an inspiration from war of course.

This device is simply a blunt-ended hollow tube with large-ish side holes. I simply put it in the anus, twist it gently to allow the mucosa to herniate through and then shave it with an 11 blade from within the bullet. I’m still fine tuning the design (i.e. making the holes ever bigger). Success in taking good enough samples is variable but I have not had any significant complications with it.
One of the lessons that I came to learn is that even in wartime children will always be children. One case that poignantly points this out is the 2 year old I had where a bullet had crossed through her torso. The entry point was in the left buttock and exit point , through the right flank. She did not look unstable and the abdomen was what you would expect in a frightened 2 years old.

On her abdominal Xray there was a foreign body in her pelvis. The maths did not add up (entry + exit point + retained foreign body) but in the circumstances I decided to operate. Upon laparotomy it turned out to be a small swallowed metal bead in her rectum but the abdomen was otherwise clean and it turned out that the bullet had a subcutaneous trajectory. She was rather lucky.
Being a doctor in wartime is a big responsibility and a privilege. War brings up a lot of moral and political dilemmas but ultimately everyone agrees that treating children can never be wrong. Children don’t even have a “side” to speak of. In times of big events I have learnt it is better to keep focused on what you can change, which for paediatric surgeon is an easy answer. Perhaps one of the main reasons that made me go back is the realization that this is a once in a life-time event. In 20 years time I could look back and think that I did what I could or simply have a safe retirement and live with the regret of the opportunity lost. I have certainly grown as a person and a surgeon during the last few years. I also came to appreciate the specialty I’m in and the training I had. I think UK training is wide and long enough to allow a solid skill base and maturity that could be used to adapt to a lot of situations. It will never prepare you for everything but I certainly think the British training system is the best in the world (I have also been through American and Syrian systems).
Finally, I’d want to highlight the fact that a lot of the work we do is supported by some fantastic UK based charities. Two of them do stand out: Syria Relief that is headed by some British Syrian Doctors and Hand in Hand for Syria. If you feel you want to donate these are safe avenues for your money. We also take in used medical equipments (including stuff with expired use by date). In fact we can make use of pretty much anything.
Muhammad Eyad Ba’Ath FRCS (Paeds) – Consultant Paediatric Surgeon, September 2017<./3>
If you would like to donate equipment please get in touch with the office and we will put you in touch with Muhammad.